Development of contextual learning models through collaboration between lecturers, students, and village governments in nursing education
Article information

Abstract
Purpose
This study aims to develop a contextual learning model through a collaboration between lecturers, students, and the village government for nursing education.
Methods
This study used a qualitative design. The process of collecting the data was done through focus group discussions with 12 informants representing four stakeholders. There were four focus groups, namely universities, village governments, community health centers, and students. The discussion used open-ended questions that were developed through two parameters, the learning outcomes and learning activities. The data analysis undertaken used thematic analysis specifically.
Results
There were 11 grouped concepts found in this study which were able to be divided into three categories. The learning outcome category was formed of four concepts, including attitudes, mastery of knowledge, skills, and values. The learning process category was formed of five concepts, namely learning resources, learning methods and forms, learning media, learning time, and learning subjects. The main sources of contextual learning were found to be programs and maternal and child health (MCH) issues in the village. Techniques and instruments were the two concepts in the assessment category. A collaboration between lecturers and the village government to help students and to provide learning resources in the village integrates the program (MCH) with the learning outcomes.
Conclusion
These concepts are the initial framework to help the head of the study program to integrate the MCH programs and cases in the curriculum and to facilitate the contextualization of the knowledge from the nursing students.
Introduction
The increasing complexity of healthcare requires nursing education programs to consider new learning strategies. Experiential learning provides a blueprint for preparing nurses for practice in the 21st century [1]. The challenges facing health students today include significant lifestyle changes and the corresponding impact on professional progress [2]. A previous study showed that most undergraduate nursing students have experienced academic burnout and that more than half had low levels of cynicism and moderately low professional efficacy [3]. Another study stated that academic burden is the main source of stress and that this is related to the number of materials, assignments, or courses required of nursing students [4]. Studies on nursing students in China show that fatigue symptoms are more common in senior students when they are in their third and fourth years [5].
It is now common practice to give nursing students a significant competitive advantage due to the intense competition for nursing staff. To maintain a balance between theory and practice, they must be able to properly put theory into practice. Nursing as a scientific discipline has its differences from other health professions, especially as the competencies to be developed must be adequate within a dynamic nursing practice [6]. Unlike other countries in the world, nursing in Indonesia began to improve in terms of education, practice, and research after 2010, especially after the declaration of the Indonesian Nursing Law. Nurses then faced a new problem, namely the gap between practice and education. The development of practice and education cannot be separated. The nursing education curriculum was developed from a technical orientation without a process to link it to competency-based nursing [7].
The implementation of the nursing process requires a contextual-based learning model (CBL). A study on the transition to a context-based learning curriculum conducted in a nursing faculty state that when implementing a CBL, four things need to be considered: adaptation, trusting the CBL process, the process of student maturity, and the controversy associated with CBL [8]. A proof of contextual learning approach highlighted student understanding, learning outcomes, learning motivation, learning attitude, flow experience, and the tendency to think critically better/higher than those who learn with conventional learning [9].
The implementation of learning in nursing education currently uses a competency-based curriculum that is divided into eight semesters in the undergraduate study program and two semesters in the nursing profession study program. The problem that is developing at this time is that the rate of not passing the Competency Test (re-taking required) is still tending to be high (above 50%) [10]. Nursing education in Indonesia has developed well. However, it is still lagging behind in comparison to other countries. Education and practice gaps need more attention, including knowledge, education systems, training, and assessment [7,9,11].
At the beginning of 2020, the Indonesian Ministry of Education and Culture imposed a new policy in the field of higher education through the “Independent Learning–Independent Campus or Merdeka Belajar-Kampus Merdeka (ILIC or MBKM)” program. The MBKM policy provides opportunities for students to gain a wider learning experience and new competencies through several learning activities outside of their study program with the hope that in the future, they can produce graduates who are ready to conquer the increasingly complex challenges of life in the 21st century. The MBKM policy is also expected to increase the link between higher education graduates and the business and industrial world, as well as the rapidly changing future [12].
One of the learning activities outside the study program can be carried out through direct practice in rural areas. This is based on the fact that the majority of Indonesia’s population resides in rural areas. Direct learning activities in rural areas are expected to foster community participation in developing villages according to the community’s needs. Rural-based development is urgently needed to strengthen the foundation of the country’s economy, accelerate poverty alleviation, and reduce the development disparities between regions. Rural areas must be seen as an inseparable part of urban areas because Indonesia’s overall development is actually about generating village potential as a source of national progress [13].
In particular, development in the health sector also requires community participation as a subject of development. The challenge is that until now, there has been no research that explains how the learning model for nursing undergraduates is implemented in rural areas. So far, the practice for nursing students has focused more on the clinical learning environment. The pedagogical atmosphere of the practice room and the role of nursing lecturers both make a major contribution to creating a conducive clinical learning environment [14]. Learning activities through clinical projects provide nursing students with the essential knowledge to provide evidence-based care. Hands-on experience makes the students aware of the importance of keeping themselves up to date with the latest knowledge [15].
The educational approach based on constructive theory emphasizes learning activities in constructing new knowledge [16]. This approach is very relevant to the CBL approach. CBL emphasizes the process of connecting the material taught to real-world situations and encourages students to make connections between knowledge and its application in everyday life [17]. Contextual learning theory is therefore the right theory that can be used to help develop practical competence. Contextual learning also provides students with practical experience in the outcome-based curriculum that is currently used by the College of Nursing.
So far, the study program uses a curriculum that has been approved by the association of nursing education in Indonesia. The curriculum is divided into two programs, namely academic and professional curriculum [18]. The weakness of the curriculum is the lack of direct learning applications in the community or clinics during the academic learning process, so students do not get real experience in how to interact with the community and patients. New students will get real experience in the clinic when taking a professional program. Based on this data, contextual model learning can be a solution to improve students’ abilities. This model allows students to interact with the community directly and strengthens the stimulation of communication competence.
This study aimed to develop a collaborative contextual learning model between lecturers, students, and village governments for nursing education. The model development focused on the learning outcomes, the learning process (pedagogical atmosphere and hands-on experiences carried out in practice in rural areas), and the assessment.
Methods
This study used a qualitative design. The data collection process was carried out using focus group discussions (FGD) to find out the responses of the stakeholders to the issue of the learning process that would be carried out outside universities and setting the further learning area as the rural areas in the province of East Java, Indonesia. This rural area was chosen to accelerate the implementation of the MBKM program as it is focused on village development. The issue raised is learning about maternal and child health (MCH) because MCH is still a priority for health programs in rural areas. MCH deals with important issues as part of realizing quality resources.
The learning environment where the research was conducted was Kemuning Lor Village. The area consists of 1,087.68 Ha located at an altitude of 150–750 above sea level with temperatures between 18°C–29°C. The population of Kemuning Lor Village in 2021 was 8,122 people consisting of 3,359 men, 4,763 women, and 741 households. Kemuning Lor village is known as an agrarian village and it has prospective natural potential for regional economic development at the village level. The problem in Kemuning Lor village is the relatively low socioeconomic conditions of the community including poverty, high unemployment, low health status, and low purchasing power being held by the people.
This learning activity is carried out in a rural community environment with very complex characteristics. There are 53 pregnant women with one person experiencing less energy protein and two pregnant women with a high risk of pregnancy. In addition, there are 218 people with data on toddlers aged 0–23 months, with a stunting risk of 56 children, stunting has been detected for seven children. Difficult access to drinking water and limited family latrines are also problems in the learning target areas. Some areas that can be targeted for contextual learning activities in the area are integrated service posts, community health centers (CHC), assistant integrated CHC, healthy village houses, early childhood education, and kindergarten education [19].
This study involved 12 informants who were divided into four groups, including the village government group, the CHC, the college group, and the student group. The village government group was represented by the village head, the head of the village youth organization, and the head of the village community empowerment cadre. The public health center was represented by the head of the health promotion section, the coordinating midwife for the public health center, and the village midwife. The higher education group was represented by the head of the Nursing Science study program, the head of the research and community service institutions, and lecturer representatives. The student groups were represented by seventh-semester students who had attended real work lectures. The average age of informants was 38.5 years old, with a minimum age of 22 years old, and a maximum age of 52 years old. Seven women and five men had a minimum of 2 years of service in their respective units and a maximum length of service of 30 years. The average years of service were 11.4 years. The informants who were students had all taken 124 credits.
Because this study was conducted during the coronavirus disease 2019 pandemic, the direct data collection process was limited, so FGD was carried out in virtual synchrony through online media. Each group was provided with one facilitator and one note-taker to compile a transcript of the recorded results. The FGD process in small groups lasted between 90–100 minutes. The discussion used an open statement that was developed based on three parameters, namely learning outcome, learning process, and learning assessment. The FGD guidelines were used to ensure that the data collection through discussions was carried out according to the procedure. At the end of the group discussion, a panel meeting was held to confirm and validate the results of the discussions in each group. The trigger questions in the FGD can be seen in Table 1.
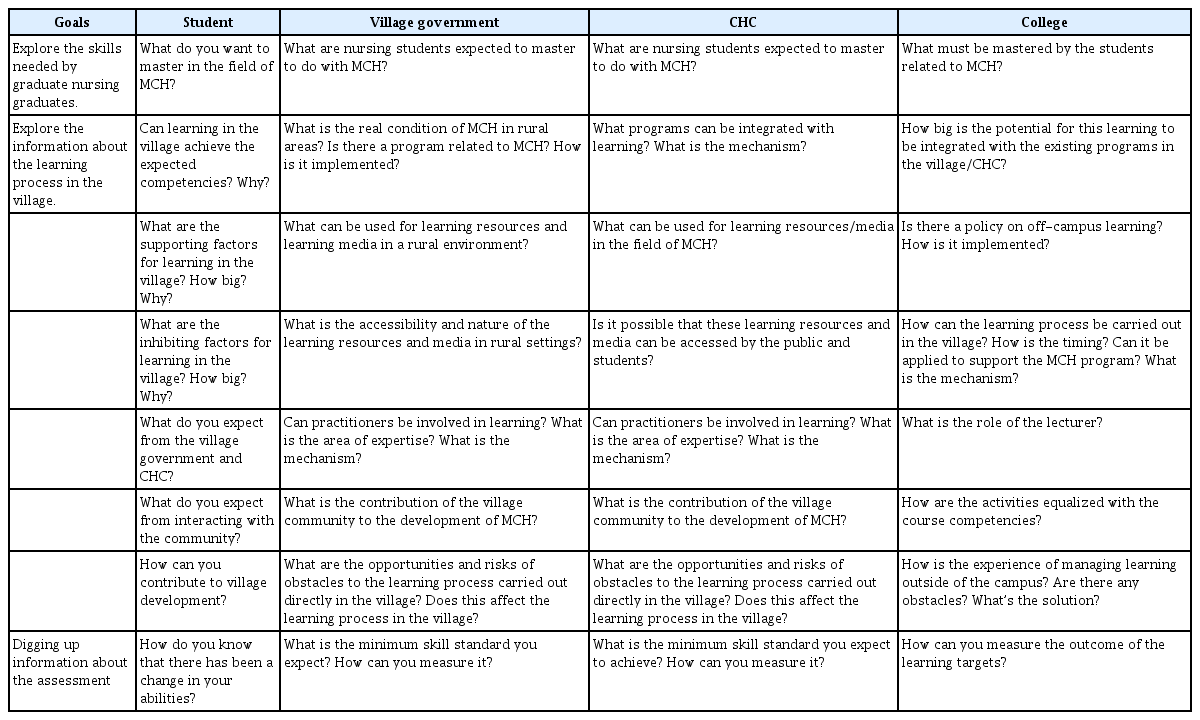
List of Trigger Questions in the Focus Group Discussions
The data validity test was carried out in the form of a credibility test involving two techniques, namely the triangulation of the data sources and the triangulation of the data collection techniques. The triangulation of the sources to test the credibility of the data was done by checking the data obtained from the village government, CHC, and universities. The data from the three sources were described and categorized (same, different, and specific views). The conclusions from the three data sources have been mutually agreed upon (member check). The triangulation of the data collection techniques was executed to test the credibility of the data by checking the data from the data sources using different techniques. The data from the village government was cross-checked with the study of the village profile document and the developing village index in 2021. The data from the universities was cross-checked with the 2021 nursing study program curriculum document, 2020 research and community service guidelines, and questionnaires addressed to the students.
The data analysis used four stages. The first stage was a complete transcript of the results of the discussion, then engaging in coding to identify the keywords. The second stage was concept formation. The researchers collected codes that were similar in content and allowed the data to be grouped into categories that related to one another, forming concepts. The third stage was categorization, namely grouping together the concepts related to the formation of the model. The fourth stage of model formation was explaining the relationship between the concepts. The framework used when developing the learning model used a backward design to determine the desired end goal first before determining the learning activities and assessments used. The description of the stages of the research method can be seen in Fig. 1.
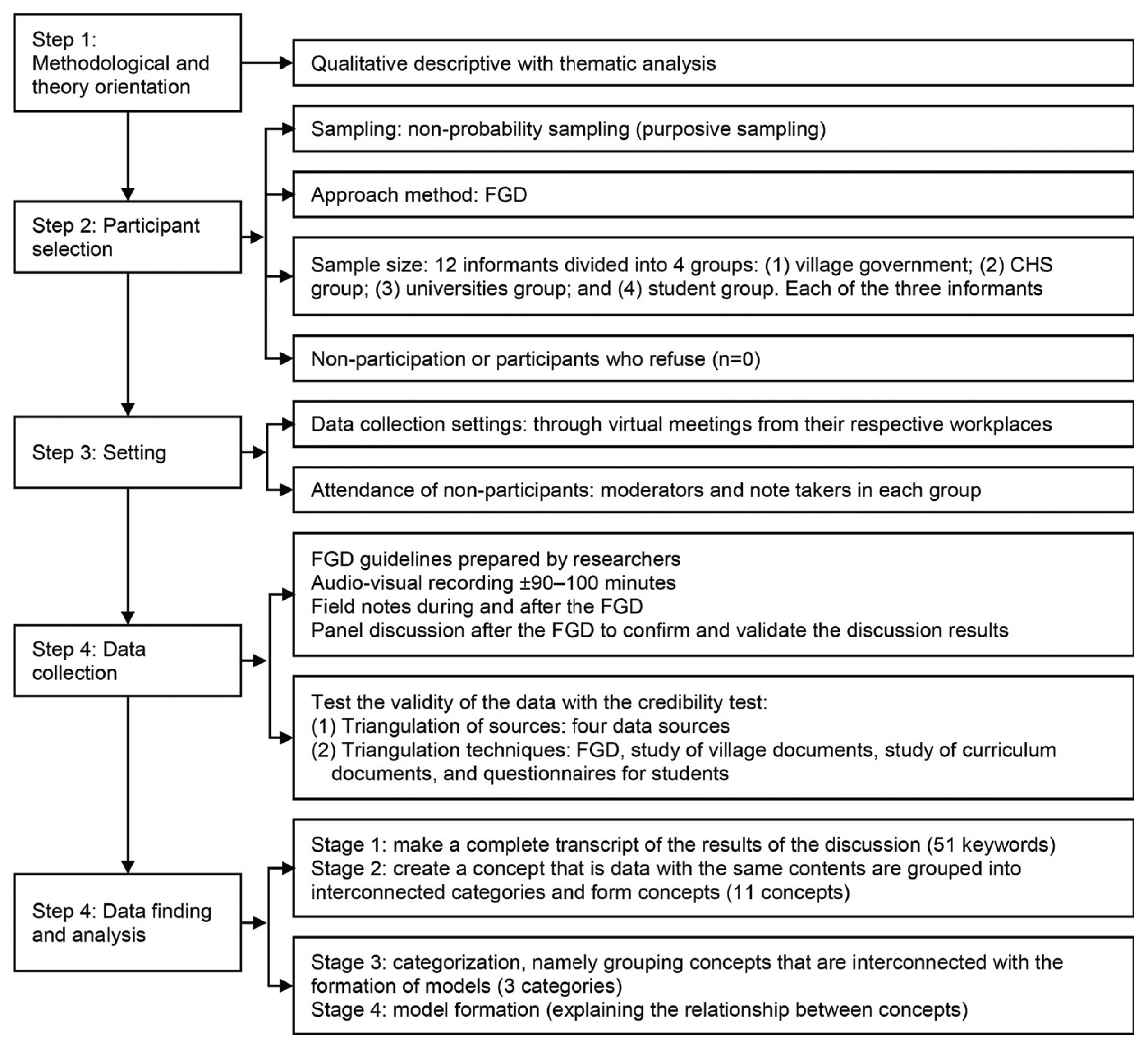
Stages of the Research Method
CHC: Community health center, FGD: Focus group discussions.
The ethical approval for this research came from the Health Research Ethics Commission of the Faculty of Health, Universitas Muhammadiyah Jember. The certificate for passing the ethical review was number 0057/KEPK/FIKES/I/2022.
Results
The first stage of analysis identified 51 keywords. The keywords were grouped based on similarities in content to form a concept. The second stage of the analysis resulted in 11 concepts. Interrelated concepts were organized into a category. The third stage of the analysis resulted in three categorizations including the learning outcomes, learning processes, and assessments.
1. Learning outcomes
Learning outcomes are educational goals consisting of statements about what the students are expected to know, understand, and be able to do after completing a period of learning. The results of this study indicate that the learning outcome category was formed by four concepts including attitudes, mastery of knowledge, skills, and values. The informants revealed the skills needed by nursing graduates when solving health problems in the village. The informants said:
“Students need public speaking skills, establishing cross-sectoral collaboration, baby care skills such as baby massage, and making making complementary food for breast milk following local wisdom. Students can also educate with local traditional healers to be able to share knowledge.” (PT1)
“Students practicing at the CHC must be able to carry out health education or promotion⋯ usually the schedule adjusts to the Integrated Healthcare Center schedule.” (PKM1)
“Some student targets, yes… according to their respective rooms. In the MCH room, it is Mother and Child Health competence, but generally in the field. On average, the practice in the field is rarely available at the public health center, so usually, brothers and sisters participate in our activities in the field such as Integrated Healthcare Center.” (PKM2).
The keywords and concepts in the learning outcome category can be seen in Fig. 2.
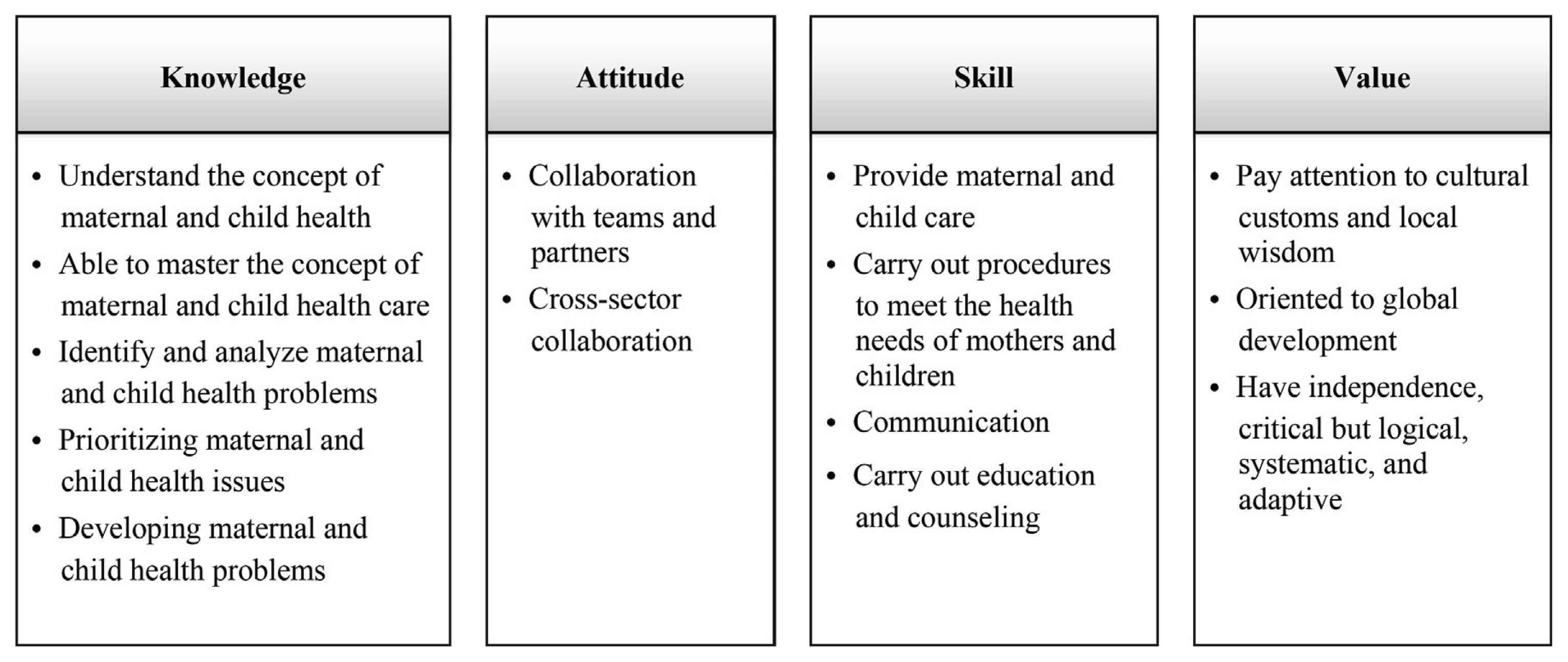
Learning Outcomes Category
The learning process category was formed by five concepts, specifically learning resources, learning methods and forms, learning media, learning time, and learning subjects. Some important keywords regarding the concept of learning resources include the variety of contextual problems that occur in mothers and children in the village. The informants revealed that MCH problems and programs can be used as a source of learning and learning activities that the nursing undergraduates can engage with when solving health problems in the village. The informants said:
“This week, there were cases of post-date and pregnant women with high risk. Some of the examined geographical areas are very difficult to reach so pregnant women do not immediately check themselves in and usually check themselves in at the end of their pregnancy. The cultural element in the village as far as I know is average⋯ there are still many pregnant women whose age has not yet reached 20 years. Nutritional status of pregnant women⋯ there are still pregnant women with an arm circumference of less than 23.5. Currently, the issue that is being raised is that stunting toddlers go up.” (PKM3)
“Yes, the performance of health cadres is very active and good, besides that there are also Community Empowerment Cadre organizations (Kader Pemberdayaan Masyarakat) and Healthy Village Houses (Rumah Desa Sehat) that coordinate with Posyandu and village midwives to collect data on MCH problems in the community. village.” (PD2)
“But in remote areas usually the majority still give birth to shamans.” (PD3)
2. Learning processes
The learning process is the process of interaction between the students, educators, and learning resources in a learning environment. The results show that the concept of the learning process consists of the learning resources, the methods and forms of learning, the learning media, study time, and subjects. The keywords and concepts involved in the learning process category can be seen in Fig. 3.
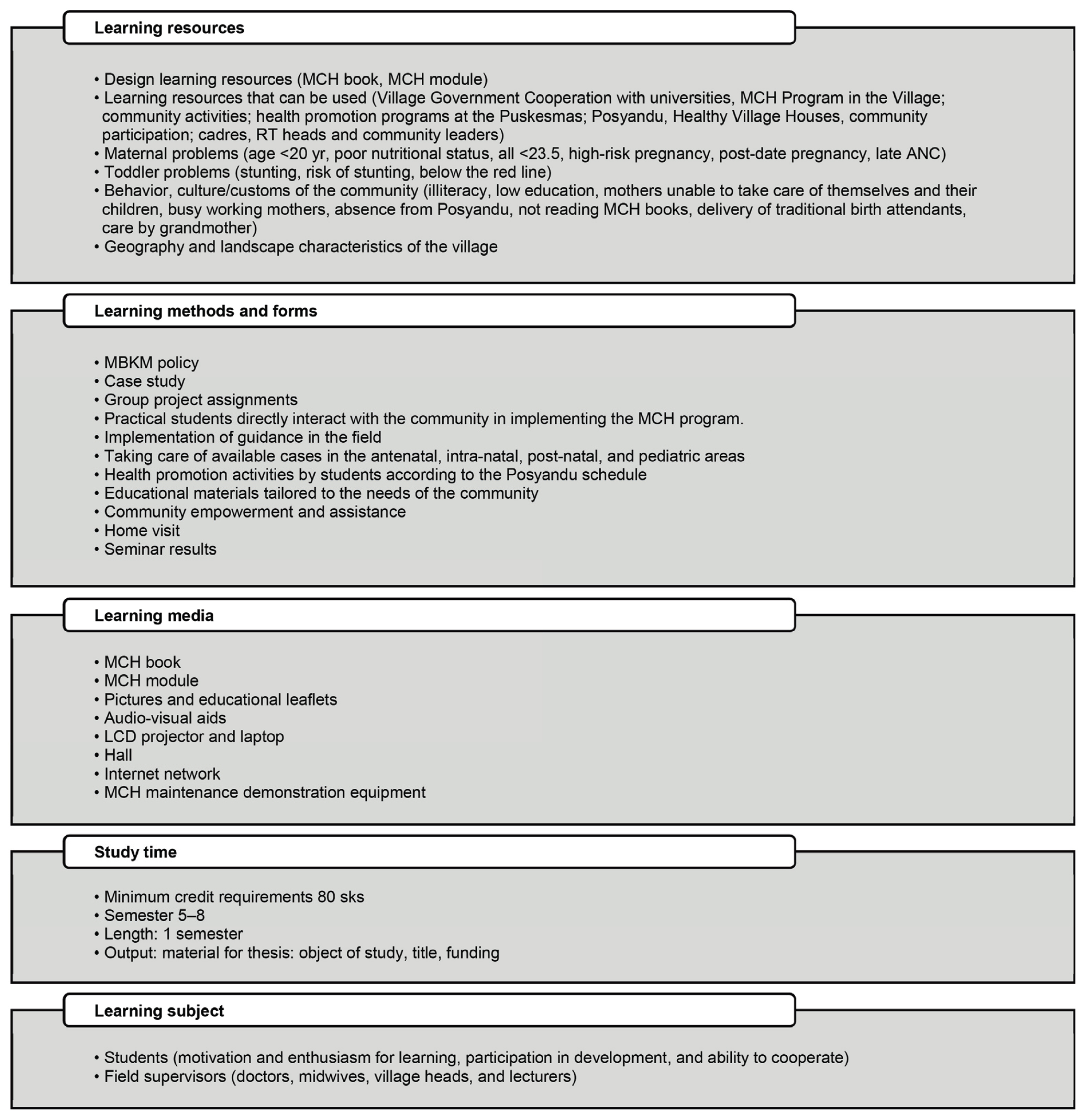
Learning Process Category
MCH: Maternal and child health, RT: Local leader of household association, ANC: Antenatal care, MBKM: Merdeka Belajar-Kampus Merdeka, SKS: Semester credit system.
3. Learning assessments
Assessment is the process of collecting and processing information to measure the achievement of student learning outcomes. The results of this study indicate that the assessment category is formed by two concepts, namely assessment techniques, and instruments. The keywords are the concepts for the assessment technique, namely oral exam, written exam, and performance. The keywords are the concepts for the assessment instrument, namely assessment rubric, observation sheets, and portfolios.
4. Model development
Based on these three categories, in the fourth stage of the analysis, a contextual learning model for building a village was developed that involves the relationship between the learning outcomes, learning processes, and assessment (Fig. 4).
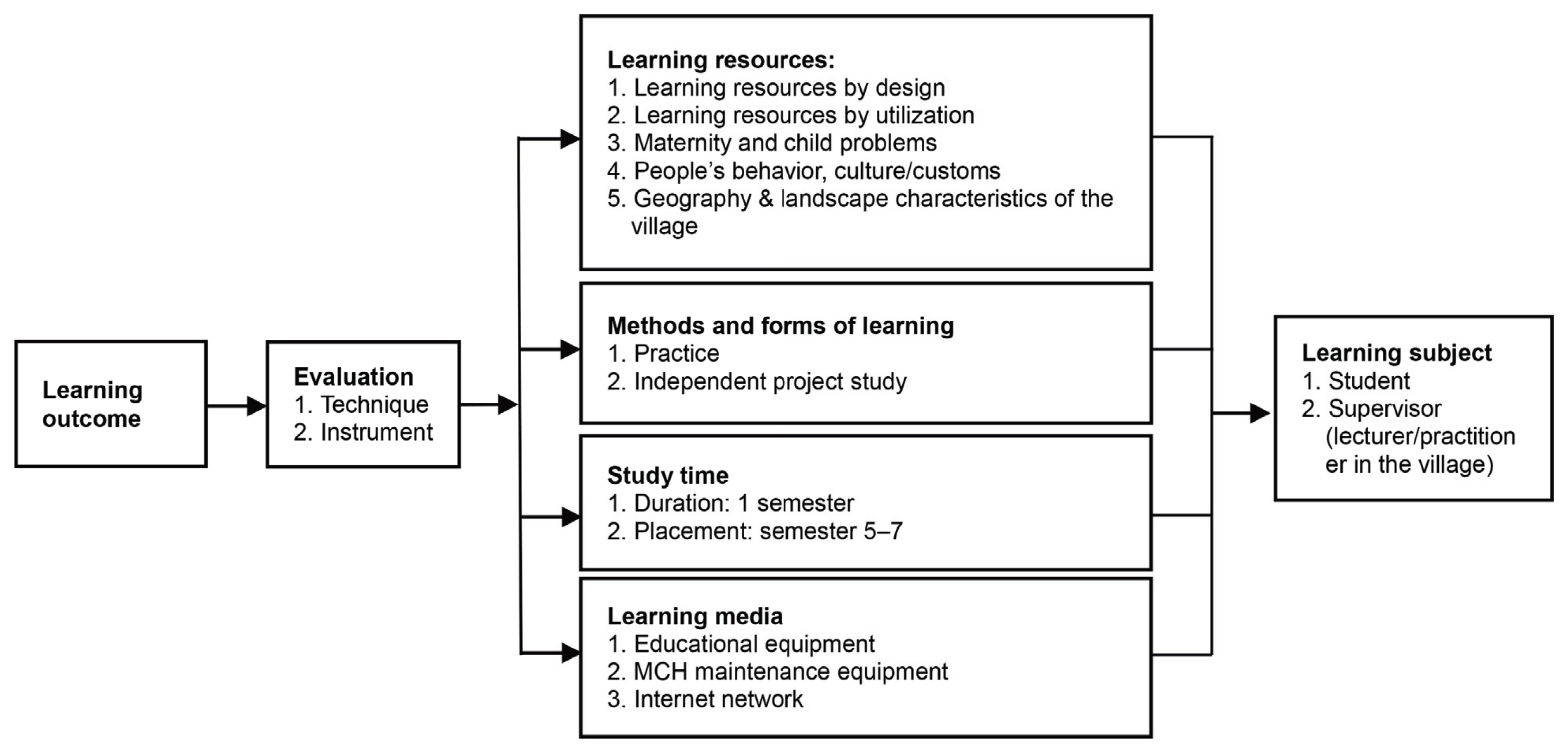
Development of a Contextual Learning Model to Build a Village
MCH: Maternal and child health.
Discussion
1. Learning outcome
The learning outcomes have revealed three aspects that must be mastered by nursing students in contextual learning in rural areas, namely the mastery of knowledge, attitudes, and skills. In addition, there is one important aspect that is needed to underlie the previous three aspects, which is value. The results of the meta-review of the studies published in academic journals from 1971 to 2016 reflect the fact that most nursing learning focuses on skills training and understanding basic knowledge. Only a few cover the domains that aim to develop the students’ higher-order thinking competencies such as solving problems and critical thinking [20]. The results of the literature review on the clinical learning environment contain four characteristic attributes that affect the learning experience and the achievement of nursing student learning outcomes, including (1) physical space, (2) psychosocial and interaction factors, (3) organizational culture, and (4) the teaching and learning components [21]. A study conducted in Iran stated that teaching methods that provide an interactive and fun environment can increase motivation to learn and lead to retention, especially in nursing skills-based programs and courses [22]. The findings of this study provide important information in that grades are achievements that must be mastered by the students. The achievement of these values guides the students when they are carrying out the learning activities. The values that are internal in nature educate the students to help them be independent, think critically and logically, and be globally oriented. External value refers to paying attention to various principles, assumptions, and beliefs that are considered good so then they become life behaviors of the community. Students pay attention to values in society so then they can build good relationships within the community.
2. Learning process
An important finding in this study relates to the variety of contextual problems that occur in mothers and children in the village and the program activities that support MCH as the main learning resources in contextual learning in rural areas. In addition to the learning resources, methods, and forms of learning, the learning media, study time, and learning subjects are concepts to do with the overall learning process. A study conducted in Kalimantan, Indonesia, found that the nursing student learning model was built on achievement and motivation to learn. Motivation is influenced by the character of the lecturer and the learning barriers that the students have. To achieve optimal learning quality, nursing students must have enough support to increase their independence and activities in the learning process [23].
Other studies have shown that experiential learning maximizes learning and makes learning more meaningful. Direct learning based on experience also allows for the achievement of goals. Direct experiential learning promotes critical thinking and self-directed learning strategies. Nursing is a practice-based profession. Therefore, experience-based learning theory and direct experience-based learning fit harmoniously with the philosophy and perspective of nursing education [1]. In addition, fostering the creativity of nursing students can be done through the activities of exposure, investigation, discovery, reflection, and evaluation [24]. A narrative study also suggested that learning strategies can increase the active participation of nursing students in the learning process. These strategies include technology-based strategies, collaborative strategies, simulation-based strategies, research-based strategies, and other learning strategies [25]. Learning aid methods, motivation, autonomy, responsibility, emotional support, and relational bonding are the factors involved in successful mentoring that is a part of mentor-mentee activities [26].
The findings of this study provide information indicating that the direct learning process in the village allows the students to interact directly with various real learning resources. MCH problems are generally obtained from textbooks or digital publications. While studying in the village, the learning resources become wider in the form of real cases that occur in the community. Learning resources involving real cases allow the students to construct and form new knowledge based on the experience of investigating cases directly. New knowledge that is formed as a result of the construction itself will be easier to remember and use in everyday life.
3. Learning assessments
The findings of this study also show the importance of various evaluation techniques in the form of both tests and tests. Through a formative assessment, students can utilize metacognition by learning what content they understand or do not understand. The integration of lessons and assessments is maximized by completing the assessments and explanations of the answers directly from the instructor [27]. A study conducted at Medical College, Navi Mumbai, in India showed that students who participated in active learning strategies helped voice their ideas independently. They were more effective in groups and increased their acceptance of the ideas/views presented in the group [28]. Providing constructive feedback in a problem-based learning (PBL) tutorial has been shown to facilitate cognitive and behavioral changes for both the students and tutors during and after the PBL tutorial [29].
Learning assessment is an important activity in the learning cycle. The assessment technique is a mechanism used to measure the success of the learning outcomes. This technique requires an appropriate instrument so then it is able to measure what it is supposed to measure.
4. Learning model development
Model development starts with the identification of the learning outcomes. The specified learning outcomes become the basis for determining the evaluation techniques and instruments used to measure said learning outcomes. Furthermore, the learning resources available in the village become an important consideration when determining the learning method to be used. Off-campus learning methods also require support from the learning media. Learning media should be relevant to the chosen learning method and available learning resources. Furthermore, the lecturers, practitioners, and students as the learning subjects are the inputs of the learning process. This model provides the practical picture that learning outcomes are the end of learning success claims. If the learning outcome has not been maximized, there is a need to re-identify the assessment system and the learning process. Has this been done well/not yet, for example? If the learning process cannot be carried out properly, the competence of the lecturers and practitioners when carrying out the learning process must be rechecked. Included here are the basic abilities of the students when participating in learning.
5. Implication
The important findings in this study include, the learning outcomes are not enough just with knowledge, attitudes, and skills. The learning and knowledge available must also be comprehensive, including values and the cultural wisdom of the local community. Rural landscapes and community cultures are good sources of learning to study MCH more comprehensively.
6. Limitations
The location of this research being in a rural area with the majority of the population being agrarian meant that the results of this study can only be generalized to similar areas. The issues explored in this study focused on MCH and are not yet associated with health issues found in both adults and the elderly.
7. Conclusion
This research has found there to be three categories formed from 11 concepts. The learning outcome category was formed by four concepts, including attitudes, mastery of knowledge, skills, and values. The learning process category was formed by five concepts, namely learning resources, learning methods and forms, learning media, learning time, and learning subjects. The main learning resources were programs and MCH problems in the village. Techniques and instruments were two concepts in the assessment category. Collaboration between the lecturers and village government students and learning resources in the village integrates the program MCH with the learning outcomes. These concepts are the initial framework for the head of the study program to integrate maternally and child health programs and cases in the curriculum and to facilitate the contextualization of the nursing student knowledge.
8. Recommendation
Further research is needed as follows: (1) It is possible to extend the setting area in rural areas to the character of fishermen and the other coast or urban areas in industrial communities. (2) The issues developed can be extended to the health sector for adults and the elderly.
Acknowledgements
We would like to thank the Ministry of Education, Culture, Research and Technology, the Directorate General of Higher Education, Research and Technology of the Republic of Indonesia, and the Lembaga Pengelola Dana Pendidikan (LPDP). We would also like to thank the Lembaga Penelitian dan Pengabdian Masyarakat, Universitas Muhammadiyah Jember, Kemuning Lor Arjasa Village, East Java, and the Faculty of Health Sciences, Universitas Muhammadiyah Jember. The author guarantees that there will be no conflict of interest either related to the research process or the interests of third parties. This research is also free from plagiarism.
Notes
Conflicts of interest: No potential conflict of interest relevant to this article was reported.
Author contributions: Drafting research ideas: NR; designing questionnaires: NR; data collection: AA, ICD; analysis and interpretation of results: NR, AA; manuscript draft: NR; manuscript review: NR, AA; supervising: NR, AA; and all authors read and agreed on the final version of the manuscript.
Funding: This research received grant support from the Ministry of Education, Culture, Research and Technology, Directorate General of Higher Education, Research, and Technology of the Republic of Indonesia through the LPDP.