Beyond the surface: unraveling global health curriculum insights through interviews of learners and educators using the CIPP model
Article information

Abstract
Purpose
Our study aimed to delve beyond a surface-level understanding and explore the various dimensions of the global health curriculum from the perspective of both learners and educators using the Context, Input, Process, and Product (CIPP) model.
Methods
From 2020 to 2021, interviews were conducted with a total of 10 individuals, including five students who had taken at least one elective course and at least one elective research course, three teaching assistants (TA), and two faculty members who had taken more than four global health courses in multiple phases in the global health curriculum. Semi-structured interview questions based on the CIPP model were used and qualitative data were analyzed through content analysis.
Results
The study identified 12 sub-themes. Students held idealized views of global health careers and sought to bridge the gap through global health classes. They desired early exposure to global health courses, emphasizing both pre-medical and clinical phases. Challenges in adjusting course difficulty and recruiting faculty were identified, along with a preference for interactive teaching methods and offline discussions. The curriculum promoted reflection on medicine’s essence, expanded career perspectives, and emphasized competencies like altruism, communication skills, and crisis management in the evolving global health landscape.
Conclusion
This study showed that a comprehensive approach is possible from the perspective of learners and educators by identifying strengths, weaknesses, and the value of the curriculum’s goals, plans, implementations, and results through the CIPP model. For optimal curriculum design, a sequential approach from basic to advanced courses is essential, promoting hands-on global health experiences for students.
Introduction
Globalization has presented various health challenges that extend beyond the boundaries of individual countries. In this era of globalization, society expects doctors not only to possess knowledge about diverse diseases and emerging global infections like coronavirus disease 2019 (COVID-19) but also to effectively treat and manage them. Consequently, the demand for global health competency among future doctors has increased [1-3].
Considering these trends, active research is being conducted in the United Kingdom, the United States, and Canada. Studies have focused on assessing student competencies, exploring experiential learning in educational methods [4-7], and developing tailored global health education programs based on student demand [8,9]. However, there is a dearth of research specifically evaluating the global health curriculum itself.
Seoul National University College of Medicine incorporated global health as the newest component in its curriculum in 2016, effectively integrating global perspectives into medical education. Despite the growing need for research on the effectiveness and assessment of the domestic global health curriculum, the existing literature primarily consists of quantitative studies focusing on class satisfaction and academic achievement [10], with a noticeable lack of comprehensive investigations. To address this gap, a comprehensive evaluation tool—namely, the Context, Input, Process, and Product (CIPP) model—was employed to assess multiple dimensions of the curriculum, going beyond mere measurements to gain a deeper understanding of its successes and shortcomings.
This study explored the global health curriculum from various perspectives beyond a superficial understanding using the CIPP model. Through interviews with educators and learners who participated in the curriculum, we aimed to uncover valuable information regarding the curriculum’s strengths, weaknesses, and areas for improvement, facilitating a comprehensive evaluation of its effectiveness and implications.
Methods
1. Seoul National University College of Medicine Global Health Curriculum
Seoul National University College of Medicine developed the “2016 Lee Jong-wook Curriculum” to infuse a global perspective into the educational objectives of the medical school. This curriculum was implemented to further the legacy of Lee Jong-wook, a graduate of Seoul National University College of Medicine and former general director of World Health Organization (WHO). The global health curriculum consists of required, elective, and elective research courses in three phases from the first year of the pre-medical phase to the last year of the clinical phase. The details are provided in Table 1.
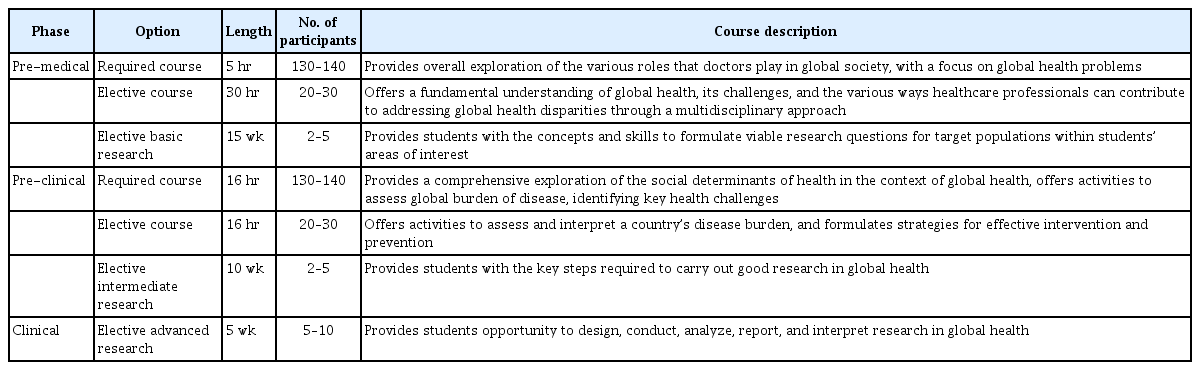
Global Health Curriculum at Seoul Medical University College of Medicine
2. Participants
Students who participated in at least one elective course and one elective research course were chosen. Teaching assistants (TAs) and professors were selected from those who participated in more than four courses in multiple phases in the curriculum at the Seoul National University College of Medicine during 2020 to 2021. Five out of 10 eligible students, three out of seven eligible TAs, and two out of two eligible faculty members participated in this study. In total, 10 participants took part in in-depth interviews, consisting of five students, three TAs, and two faculty members (Table 2). The TAs were researchers at the JW LEE Center for Global Medicine, majoring in global health or having experience in the field of global health. A faculty member was defined as a full-time professor who was active in the global health field and affiliated with JW LEE Center for Global Medicine. Participants provided consent based on the information provided. Since interview data were collected as part of a regularly conducted curriculum evaluation and the interview script did not contain personal information, the Institutional Review Board of Seoul National University College of Medicine and Seoul National University Hospital exempted this study from review (E-2306-144-1441).
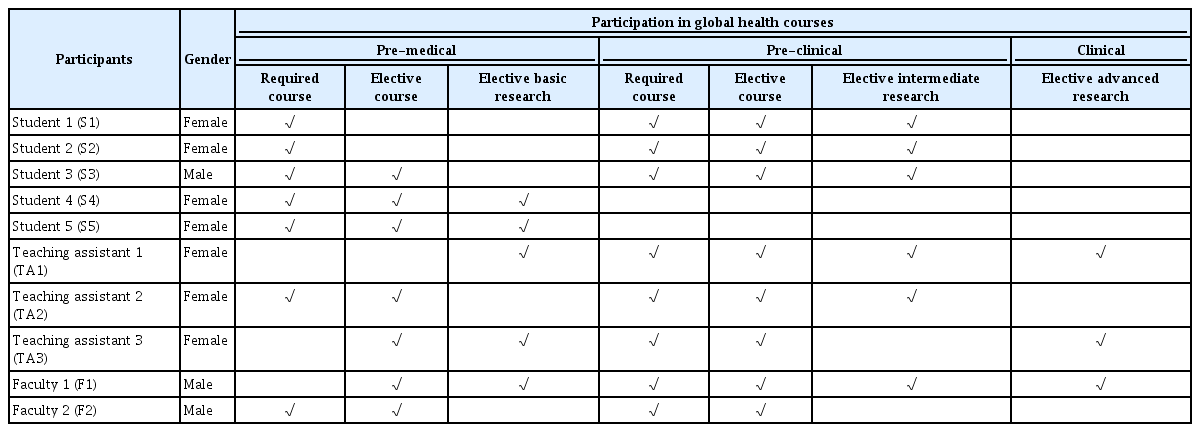
Basic Information of Participants
3. Data collection and analysis
The researchers conducted the interviews by meeting the participants in person or remotely via Zoom meetings as part of the course evaluation for approximately 60 minutes. Participants provided informed consent based on the information provided, and anonymity was ensured. The interview questions were semi-structured and based on the CIPP model, with topics such as expectations of the courses, composition of the curriculum, preparation of curriculum, teaching method, and outcome of the curriculum. Data were collected from January 2022 to April 2022. Data analysis was performed by subject using ATLAS.ti (https://atlasti.com/) and the content analysis model [11]. After two coders checked and coded the interview transcripts, they discussed possible sub-themes several times before deriving the sub-themes and used an inductive method of placing themes according to the CIPP model. The final draft was finalized using the triangulation method [12], in which a third party independently re-examined and validated the derived sub-themes and themes, thereby ensuring the robustness and reliability of the analysis.
Results
Twelve sub-themes were identified through the CIPP model. Table 3 summarizes the results of our study.

Results of In-Depth Interviews Using the CIPP Model with Content Analysis
1. Context
Global health opportunities, such as those offered by organizations such as WHO and Médecins Sans Frontières (MSF), are initially regarded as prestigious and intriguing by many students. To bridge the gap between their vague imaginations and the reality of global health, students actively seek out global health courses. They are eager to expand their existing thoughts and gain a deeper understanding of how the field truly operates, going beyond their initial idealized notions.
I vaguely imagined what global health would be. So, I want to break through from the ideal…most people think of Doctors Without Borders or activities that look fancy when they imagine global health. (S4)
Global health was often idealized, yet many students lacked a clear understanding of its reality and applicability in their medical careers. Limited information and a lack of global health courses in the medical school curriculum worsened this knowledge gap. Students were eager to explore the scope and meaning of global health, particularly how it could intersect with their future roles as medical students or doctors. To address these concerns, students expressed a desire to hear real stories and experiences from professionals actively engaged in the global health field. They sought mentorship and guidance to understand the diverse paths and opportunities available. Educators recognized the importance of encouraging students to think about their own roles and participation in global health, aligning with the educational goals of fostering global perspectives and leadership skills.
There are not many global health classes in the medical school curriculum. (S1)
There is no clear role model, no consented education approach… the goal is to create an environment where students can recognize and be exposed frequently. (F1)
I try to make it possible for students to consider various roles of doctors in universities and hospitals around the world, and it also relates to our educational goal and graduation competency. (F2)
2. Input
Within the curriculum, there was an increasing demand from both educators and learners for early exposure to global health. Many comments expressed a strong desire to introduce more global health courses in the pre-medical phase and highlighted the importance of early engagement in global health.
Totally agree to open more courses in the pre-medical phase… The sooner the better for students. (TA2)
We need early exposure to global health. If we do clinical practice, global health coursework will be pushed to the background even if it is available. (S3)
By adjusting education to suit the student's development stage, learning results could be optimized and students could be properly challenged based on existing knowledge and skills. However, educators often faced difficulty in global health education because there were no clear boundaries and fixed frameworks or reference points to measure the degree of knowledge in global health field.
There are limits to what you can do in the pre-medical or pre-clinical phase. (S5)
Adjusting the difficulty level of each course is so hard because the instructor does not know how much the students know about global health, and there is no indication about how in-depth to teach it. (TA2)
Due to the expanding importance of global health, others believed that a basic knowledge of global health should be a required component, particularly considering the COVID-19 situation. However, balancing between the required course and the elective course is needed because not all students may be interested in global health.
As the importance of global health is increasing because of COVID-19, it is necessary to increase the number of required courses… The proportion of required courses is too small. (S2)
Some students are interested in global health, but some are not, so it is better to increase the number of electives. (S4)
Recognizing the importance of fostering faculty development, efforts were made to recruit qualified instructors, but it was not easy. TAs participated in class preparation process, practice, required course, and elective research to provide additional guidance and expertise to students because of the shortage of experienced instructors.
Instructors either know too much theory or only know too much practice. (TA1)
TAs always got involved in our group discussions, they observed and facilitated our discussions… they are our mentors, guidance, friends, and coordinators of our curriculum. (S4)
3. Process
Due to the nature of the subject, global health courses consisting of only simple lectures have limitations because it is important to learn not only through theory, but also through various cases and practical experiences. Various learning and teaching methods were employed, including small-group discussions, project-based learning, roleplaying, and field trips, to address these limitations.
It is impossible to take global health courses through only theoretical lectures… It is only meaningful if activity is included. (S2)
Every time I went to class, as one of the small-group members, I role-played, created news, and always took a new approach to global health… and those activities were really helpful for me to understand global health. (S4)
However, due to the COVID-19 pandemic, the planned field trip was not possible to conduct. Distance learning was conducted as an alternative, with activities including holding a roundtable with experts working at the WHO or MSF, so that learners could gain indirect experience.
If it was not for the COVID-19 pandemic, I would have gone to the site and experienced it myself, but I was able to hear a vivid voice through a roundtable discussion online with experts in Geneva, WHO. (S3)
Through distance learning, which transcends time and space, we wanted to convey to students a diverse approach to global health. (F2)
Moreover, in such large classroom settings, where student-student and student-faculty interactions can be challenging, the use of small subgroup divisions became essential for fostering active engagement. These subgroups enabled more effective interaction, and the presence of TAs played a crucial role in enhancing the quality of student-faculty and student-student interactions.
People who do not talk often do not talk until the end, but a TA came in and created an atmosphere for most people to discuss, and as a result, I think the class became fun and comfortable because we got more familiar with each other. (S2)
During the group discussion, one TA per group came in and explained in detail what I did not know during the group discussion, so I felt like I was getting intensive coaching… (S4)
I felt like I became a part of the student group by participating with the students and discussing and studying the global health. (TA3)
However, students asked to be guaranteed time to explore topics of interest and conduct self-directed learning, project-based learning or research independently, as well as time to receive feedback from faculty and to supplement and think about their strengths and weaknesses.
If I had more time, I could have fully expressed my opinion on the faculty’s feedback and explained what I thought about the design and what I based it on...think of various perspectives rather than a simple intervention. (S2)
We received numerous requests from students for extended time during project-based learning or research courses. If they had the chance to have enough time, they would think more deeply about their project. (F1)
4. Product
The curriculum prompted students to contemplate the essence of medicine and its social responsibilities, fostering their recognition of the intrinsic value associated with the role of a doctor, while also opening up new avenues for exploring a career in global health.
I really went through medical school as if I was enduring it…I felt very much that there are definitely values that exist, so I am studying now to realize those values. (S2) I felt that working in global health was not easy as a doctor, but through various cases, I came to think that I could do it. (S5)
Participants mentioned the required competencies as global health agents throughout the global health curriculum, such as altruism, communication skills, and crisis coping skills. The curriculum emphasized that these competencies were necessary for collaborating with experts, addressing global health challenges, establishing effective partnerships, and responding effectively to emergent health crises.
Altruism is the most important thing from the beneficiary’s point of view, not from the supplier’s point of view. (S2)
I think we need to learn how to increase communication and agility so that we can adapt to rapidly changing situations and recover quickly. (S4)
To enhance students’ capacity to respond to a changing world, we must develop their skills to utilize new crisis coping systems/methods. (F2)
Discussion
Our study employed qualitative research methods and the CIPP model to gain a deeper understanding of the global health curriculum by engaging various stakeholders, including learners and educators. Several topics for further consideration emerged from this study.
Firstly, despite the prevalence of discussions on globalization, there were limited opportunities to learn about global health in universities, particularly in medical schools. Despite efforts in many countries to approach global health programs in various ways that align with students’ demands and expectations [5,6,8], global health courses remain scarce [13]. This reflects a lack of consensus regarding educational methods and approaches to global health education [14]. Moreover, the absence of agreed-upon models for global health approaches in Korea could also influence the availability of global health education in medical schools [15,16].
Secondly, instructors faced challenges managing the global health curriculum. The educators grappled with defining the boundaries of global health education due to the vast and dynamic nature of the subject. There was a notable discrepancy between educators with heavy theoretical knowledge and those with mainly practical experience, suggesting a need for balanced expertise in the teaching staff. To overcome these challenges, TAs played an important role as facilitators to ensure that students received more individualized attention and developed a better understanding of global health. They bridged the gap between theory and practice, enhancing the overall learning experience [17].
Third, the COVID-19 pandemic affected the conduct of certain activities, like field trips, pushing institutions towards innovative solutions such as distance learning. This adaptation underscored the importance of flexibility and creativity in curriculum delivery, especially in ever-evolving fields like global health. A previous study reported that distance learning allowed students to share their opinions with experts and practitioners at a distance beyond the traditional classroom environment [18], and it was flexible in facilitating knowledge transfer regardless of location [19].
Fourthly, learners and educators emphasized the importance of collaboration, the identity of doctors, and shaping their career trajectory through the global health curriculum rather than solely acquiring knowledge. Through various educational methods encountered in the global health curriculum, students directly or indirectly developed their ability to cope with local situations and gained expertise from their environment [20]. This highlights the necessity of tailoring curriculum content to match the realities of the target country, prioritizing community trust and cultural adaptability [21]. Communication skills that allow flexible crisis preparedness are crucial, and both students and medical schools should be prepared to develop these capabilities in the future [22]. However, it is essential to ensure a balanced development of competencies among students, whether they are considering global health as their career path or simply have a general interest, by effectively harmonizing required and elective courses [23,24].
Lastly, the CIPP model could be applied to systematically evaluate the overall quality and structure of the curriculum. In organizing, planning, operating, and executing the curriculum, hidden problems could be discovered and appropriate improvement strategies can be derived through deep analysis at each stage [25,26]. Additionally, this model supports the continuous improvement of the curriculum by emphasizing the efficiency and connectivity of the process itself, rather than simple outcome-oriented evaluations. In this respect, the CIPP model provides diversity and depth of educational evaluations and suggests directions for improving overall educational quality.
While generalizing findings from qualitative studies requires caution, it is noteworthy that this study considered the perspectives of educators and learners, who are key stakeholders in the curriculum. Our study has provided valuable perspectives from both learners and educators, shedding light on crucial elements that contribute to a comprehensive global health curriculum. The findings from this research can serve as a valuable resource to enhance educational practices, preparing future healthcare professionals to tackle the challenges of global health.
Based on this study, the authors would like to propose suggestions to improve the global health curriculum. Firstly, efforts should be made to convene a consortium within medical schools to foster consensus on approaches and teaching methods for discussions on global health. Secondly, to provide insights and experiences in global health to medical students interested in the field, a variety of teaching methods should be utilized, enabling students to learn directly and indirectly, rather than relying solely on one-way lectures. Efforts are also needed to train instructors with expertise in the field of global health and practical experience. In cases where this is challenging, synergy can be harnessed through collaboration between professors and TAs to provide students with a balanced perspective, enhancing their overall learning experience. Finally, the curriculum should be designed to harmonize required and elective courses according to the students’ developmental stages, ensuring sufficient time for self-directed learning and professor feedback. By providing time for independent research, projects, and reflection, students can be encouraged to explore specific interests and gain in-depth knowledge.
Acknowledgements
The authors would like to acknowledge the Office of Medical Education of Seoul National University College of Medicine and JW LEE Center for Global Medicine for their ongoing support for developing, implementing, and evaluating the educational curriculum.
Notes
Funding
None.
Conflicts of interest
No potential conflict of interestrelevant to this article was reported.
Author contributions
Conceptualization: HBY, YJL; methodology: HBY, YJL; content analysis: HBY, YJL; validation: HBY, JYP; Writing–original draft preparation: YJL; writing–review and editing: HBY, WHK, JSS; and approval of final manuscript: all authors.