Introduction
Serious games are games with educational goals that are designed for a purpose other than entertainment [1]. Serious games provide a low stakes environment for learner experimentation and improvement through iterative play. They can modify learner behaviors and attitudes in service of educational goals and directly demonstrate educational content to facilitate learning. Serious games exist in many formats though much of the literature in medical education focuses on digital games; sometimes to the exclusion of tabletop games (card and board games) from the definition of serious games [2]. Board games have evidence for efficacy showing improved longer-term retention compared to traditional educational methods [3]. While the body of literature has grown, publications remain focused on implementations of single games with learner reaction data and immediate learning outcomes. Guidance regarding the ideal format including player counts, length of play, and general preferences of users are yet to be described. The goal of this study is to fill this gap and inform educators to design games to meet the needs of learners.
Methods
1. Survey development
The goal of this survey was (1) to learn what game characteristics best meet student and educators needs and (2) to understand barriers for use of games among students and educators. The study received exempt status by the Oregon Health and Science University Institutional Review Board.
Survey questions were developed based on literature of players’ perception of a game for medical education, literature outside of medical education on barriers to implementation of games in the classroom, communication with creators of tabletop games for Health Professions Education (HPE) and with educators in other disciplines who use games for teaching [4,5]. Questions were piloted in social media channels dedicated to educational games and modified based on results of this feedback for content and clarity. They subsequently were piloted on pediatric faculty members and again modified.
Complexity scale was modified from BoardGameGeek weight (complexity) ratings using examples of games falling into different ranges based on lists of popular classic and hobby games (https://boardgamegeek.com/). This scale was refined to assure that users would be familiar with at least one reference game in each category. The lowest complexity category was split into two to better reflect the landscape of current medical education games and the highest complexity range was removed due to lack of universally familiar examples. The full survey is available in Supplement 1 .
2. Survey distribution
The survey was offered to people downloading a printable card game used for medical and pharmacy education from December 13, 2021 to June 13, 2022 with the goal of surveying students and educators already interested in using games for education. This game was promoted on social media channels focused on HPE on Twitter, Facebook, and Reddit. Users who clicked a link to download the game were asked if they would like to participate in this survey prior to accessing the game.
3. Analysis
Response rate is reported as the percentage of users who submitted the survey divided by the total number of users who went to the game files. Responses of those who endorsed health profession roles were analyzed. All questions were optional and submitted surveys with current health care roles were analyzed regardless of the percentage of other questions completed. Results are described divided between those intending to use the game for teaching versus their own learning.
Results
1. Respondents
The questionnaire was submitted by 390 (23%) out of 1,717 people who went to the game files. Of these 55 were excluded as they did not specify a role in healthcare. Most were in the United States (53%) and in the physician (56%) or pharmacy (33%) domain. Most participants were downloading the game for their own education (71%) and most did not have previous experience with games for education (83%). Demographics of participants are displayed in Table 1.
2. Preferences and barriers
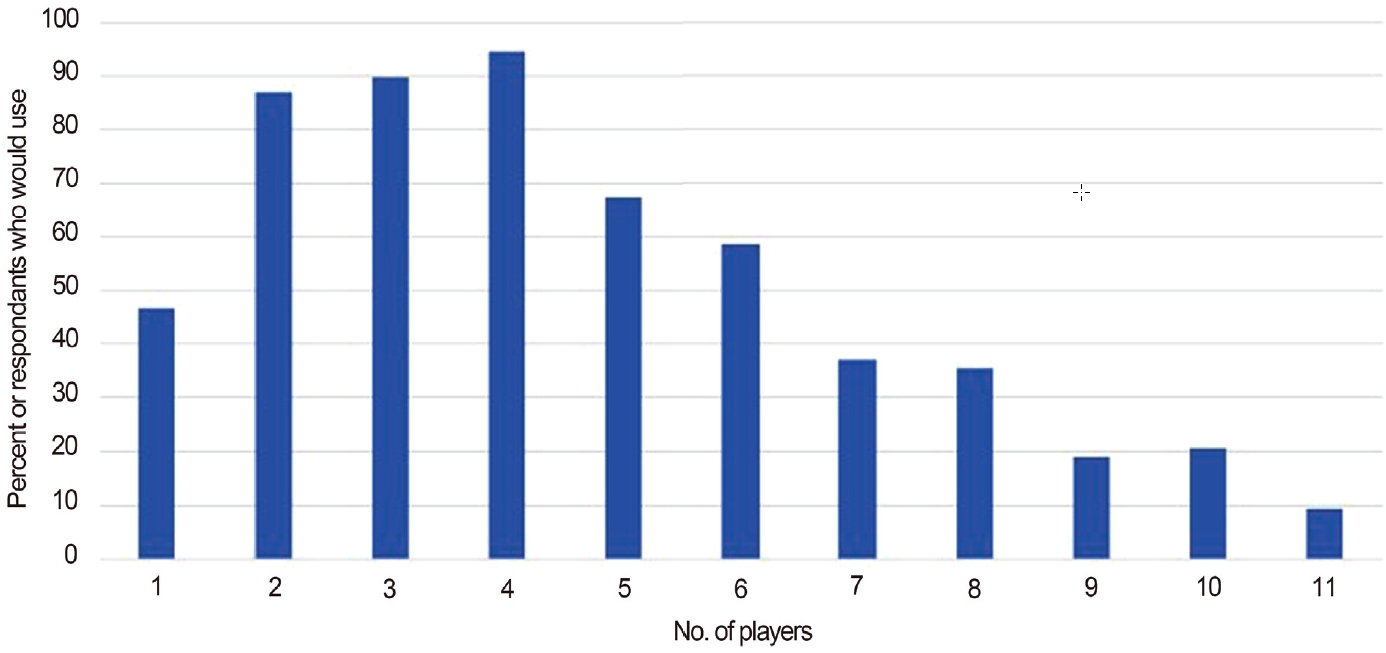
There was a preference for games with shorter play times <20 minutes or 20–39 minutes. There was also better acceptance of low to medium complexity when compared to higher complexity formats. There was not a strong preference between cooperative, competitive, team, or solo formats (Table 2). Two to four players were best accepted (Fig. 1).
The most commonly endorsed barriers to use of games for medical education were: lack of games to meet educational goals (85%), concerns about games content accuracy (70%), and cost of games (64%). Free text comments included concerns around accessibility includeing language, topic specific availability, awareness of games for education, content concerns including ability of individuals to rely on accuracy of material, and logistical challenges around implementation.
One respondent described the challenges around student confidence when using games for teaching.
“It seems like a wacky idea (although actually is a very good idea), and so I worry that I would lose the confidence of my students if I made up a game like this. A game made by somebody else, however, would look like a legitimate thing and so I would be more confident using.”
Discussion
This study provides a number of considerations for designers and users of games for HPE. Cost was highlighted by participants in our survey as it has been by others looking at users of games for HPE [6]. With the challenge of cost in mind, there are games available free to print either directly from designers (e.g., Em3.org.uk) or published as journal supplements [5].
Content accuracy is a consideration for any educational resource and was highlighted here as an important concern. Literature on online medical education suggests some strategies that could be applied to games for medical education. These include provision of and consistency with the references, clear disclosures, and the use of a defined editorial process. MedEdPortal (https://www.mededportal.org/) is one source which provides a defined peer review process for game content.
Tabletop games can be presented in a wide variety of formats, playtimes, player counts, and degrees of complexity. For example, a short low complexity card game “Clinical Coaching Cards” has been used in the setting of workshops for faculty development [5]. A more complex board game “GridlockED” is an hour or longer and is used for two to six players in a wider variety of settings [7]. When designing games length and complexity are important considerations in part driven by particulars of the educational setting. Although learners and educators generally prefer shorter games, games described in the literature are often an hour or longer. As an example, a 90-minute game was felt to be too long by some students [8]. Educators should consider using shorter games based on these findings. Shorter games allow for more time to either present material upfront or debrief after gameplay. Debriefing is important to consolidate learning and address potential misconceptions from the way reality is simplified for the purpose of a game.
Respondents preferred lower complexity games consistent with games described in the literature. Appropriate complexity varies by setting, more complex games may be appropriate in the classroom setting with less extraneous cognitive load compared to games used for teaching in the clinical setting. Additional complexity beyond what is needed to meet the educational goals comes at the cost of germane cognitive load and could be a detriment to learning. This was summarized nicely by a respondent to our survey.
“The game complexity shouldn’t be harder than the information it’s providing. The point is to learn, not to understand the game.”
Regardless of setting it is wise to minimize complexity and choose rules and mechanics that align directly with the educational goals.
There are theoretical considerations regarding the strengths and weaknesses of using competition or cooperative mechanics in educational games. For example, self-determination theory has been used to support team-based competition and raise concerns about the negative effects of individual competition [9]. We found cooperative, competitive, team, and solo games were all acceptable options to respondents.
This survey was administered to a sample of learners and educators interested in a specific free to print game “Empiric” which is a short, lower-complexity game and may have influenced the population surveyed [10]. Although the instrument was piloted among educators both with and without a game design background, no specific testing for reliability was performed.
Serious games are an innovative part of the HPE tool kit. This study describes ideal design considerations for tabletop games. Educators interested in creating their own serious games to incorporate into their teaching should target games to lower complexity and shorter play times to meet both learners’ and other educators’ preferences. While serious games are a proven way to enhance learning we have identified continued barriers to the implementation of tabletop games in HPE including a lack of games in desired content areas, the cost of existing games, and concerns about content accuracy. This study is the first step in addressing the absence of serious tabletop games for HPE. In order to make serious games a standard educational tool further research is needed to define how to assure and demonstrate content accuracy.