Introduction
With social developments, societies have changed to knowledge-centered societies that require high levels of knowledge. This change has subsequently increased the importance of the role of experts who lead social changes and developments. In general, experts are defined as those who consistently demonstrate exceptional abilities in a certain area [1]. Clinicians are also knowledge-oriented professionals who are always mentioned in the expert group.
In other words, various studies have been conducted to analyze the characteristics and components of performance or comparatively analyze the differences between novices and experts to analyze the characteristics of experts [2]. Some articles suggests that expertise requires systematic, high-intensity training of at least 10 years or 10,000 hours [3].
Many studies have also investigated the components of expertise. In particular, knowledge, experience, and problem solving constitute the most basic components of generally accepted expertise [4]. Experts perform typical activities at each of the following stages: recognizing problems, defining problems, finding solutions, carrying out solutions, and reflection [5]. In experts, conceptually more abundant and organized representations occur, allowing them to solve given problems, and experts also tend to use abstract representation relying on in-depth knowledge. Here, knowledge representation refers to knowledge that externally expresses information organized within the cognitive framework [6]. Especially, clinical experts have a high knowledge structure, and based on this understanding, experts widen and deepen the representations while focusing on the fundamental principles [7]. Decision making, which refers to the process in which problems are recognized and solutions are selected upon consideration, is also defined as a process in which one reaches their selection among various possible alternatives through complex dental cognitive processes [8].
When compared to non-experts, experts have the ability to process unnecessary information without filtering and efficient neuronal networks [9]. Clinical experts can also make accurate selections in given tasks due to their abundant experiences with the tasks [10]. In addition, studies have also suggested that experts have higher activation of the frontal lobe, which is important for cognition in experts [11], and needed for prediction and observation of behaviors, and that experts and nonexperts have different neuronal mechanisms [12,13].
The brain consists of millions of neurons, and each neuron is connected to other neurons in various interrelationships. The interaction between these neurons, which can lead to learning, memory, behavior, decision making, and recognition, occur in synapses. Here, the information is transmitted in synapses through chemical substances, particularly due to the electric potential differences created by concentration gradients across the plasma membrane. Such electric potential differences were caused electric signals on the scalp, which are measured in electroencephalography (EEG).
This study was aimed to suggest a model of brain-based experience-knowledge in order to improve clinician’s decision-making process. Clinicians’ EEG characteristics, which influence complex clinical decision-making processes, were analyzed, and a brain-based learning model to improve experts’ clinical decision making was proposed based on this.
Methods
In this study, medical experts were defined as those who have been continuously working in clinics for 10 years or more and can effectively solve problems in clinical decision-making. This study was performed in the following two projects to develop a brain-based model of experts’ experiential knowledge: (1) The first study is a qualitative study of clinical decision-making in a clinical scenario. (2) The second study is an analysis of differences in the cortical activity of experts and novices through EEG.
In the 1st study, the setting was videotaped to investigate the thought processes used for decision-making performed in a real-life clinical setting. While reviewing the videos together, the participants’ characteristics in thought processes for decision-making were deduced through the think-aloud method and focus group analysis. In the 20th century, the Wurzburg group of philosophers developed this into a new experimental method termed “introspection” in associative theories that explain human mental processes using ideas and association. Initial experiments involved free association of words and explanation of the thought processes [14,15]. And then, in order to supplement the think-aloud method, this study used focus group analysis to analyze the decision-making process in medical experts, which was the focus of this study, in more detail.
In this study, a standardized patient was recruited to reproduce clinical situations and developed a scenario for the patient based on her symptoms. This patient’s case was standardized, and all participants participated in an experiment on their decision-making process. The scenario for clinical decision making (standardized patient) is are following. “Wisdom teeth problem: The patient has been feeling discomfort in upper right molar since 2 years ago, and food sometimes gets stuck at the location after eating. With recent increases in stress from work, the symptoms at the site have worsened, and the patient feels throbbing pain.”
In the 2nd study, the three major steps established through the experiment conducted under an environment simulating the actual clinical environment were developed further into tasks to measure brain waves in the experts and novices. “Confirmation of the patient’s chief complaints,” “oral examination,” and “radiography reading” steps were developed into six tasks, and the experts’ and novices’ cortical activities were measured through a 32-channel EEG. The data measured during the six tasks were pre-processed to statistically analyze the differences between the groups.
Two sets consisting of one piece of auditory information and two pieces of visual information are presented while EEG signals are measured from each participant. Set 1 involves stimuli about an identical patient whereas set 2 involves stimuli about different patients. Here, the expert and novice dentists were asked to record, with a stopwatch, the time required for them to identify the task, identify the patient’s problem, and make a decision, in order to analyze differences in the timing of diagnosis at which a decision was made. Fig. 1 shows the overall experimental procedure.
This study was used Matlab (MATLAB 2012a; MathWorks, Natick, USA) and EEGlab (Swartz Center for Computational Neuroscience, La Jolla, USA) for noise filtering and data analysis. Data reprocessing were pre-processed to analyze the changes in EEG signals on the scalp by analyzing the differences between the two groups in terms of phase distribution of each frequency range (beta, alpha, theta, and delta bands) using EEG lab. The data preprocessing (continuing EEG) is following: data reduction (e.g., bad channels selection) → rereference → electrooculogram removal–independent component analysis (ICA) → filtering → visual inspection.
Using band pass filter by fast Fourier transform (FFT), waves with frequencies above 50 Hz were removed. This is FFT, which is often used to convert the time domain into the frequency domain, and the following equation Fig. 2 is used [16].
For each task, this study was comparatively analyzed changes in frequencies in the expert and novice dentists' decision making (diagnosis). The pre-processed data were tested for significance on IBM SPSS statistics ver. 22.0 (IBM Corp., Armonk, USA) for each task in independent samples t-tests and one-way analysis of variance. Using EEGlab, the distribution of activated cortical areas during each task for the experts and novices were comparatively analyzed.
The study protocol of the present study was approved by the Institutional Review Board of Seoul National University Dental Hospital, Seoul, Korea (CRI17006). Informed consent was obtained from all individual participants included in the study.
Results
Using the basic protocol for analysis of differences between novices and experts in each step, the transcripts of think-aloud and in-depth interviews conducted for 10 novices and 10 experts were analyzed through thematic analysis. Fig. 3 shows the characteristics in thought processes in clinical decision making in each step-in experts and novices.
The medical experts collect and interpret verbal and non-verbal information while thinking about communication from the moment they identify the patient’s chief complaints. In step 1, they establish and categorize all possible hypotheses based on experiential knowledge and evidence at the moment they identify the patient’s problem. At the same time, they perform backward reasoning of the hypotheses. Here, the experts identify facts at each step while maintaining an open mind and keeping in mind that the hypotheses might differ from the actual problem, unlike the novices. Moreover, the clinical decision in identifying the chief complaints, diagnosis, and treatment planning is performed in a simultaneous manner rather than in a stepwise manner. The experts move flexibly through all stages whenever they collect new information. Rather than organizing thoughts in the last diagnosis step, the decision-making proceeds while the clinicians converge and diverge simultaneously at each moment. However, also in this process, the clinicians make decisions closer to the definitive diagnosis during physical examination than during the chief complaints step and also while confirming radiographs than during physical examination.
In contrast, the novices focus on identifying facts and collecting information while identifying the patient’s chief complaints. The novices tended to think in a stepwise manner from testing until diagnosis. Although some novices established and categorized hypotheses based on the materials learned in classroom and their experiences when they identified the patient’s problem in step 1, most tended to focus on documenting the patient’s story. Here, the novices acted and thought according to the learned protocols and failed to think flexibly about other possibilities. The novices tended to select and establish hypotheses during physical examination rather than while identifying the patient’s chief complaints. Then, they condensed the hypotheses while confirming the radiographs to make decisions. Moreover, when problems arose, they tended to depend on other experts and to think anew rather than establishing another hypothesis and approaching the problem themselves.
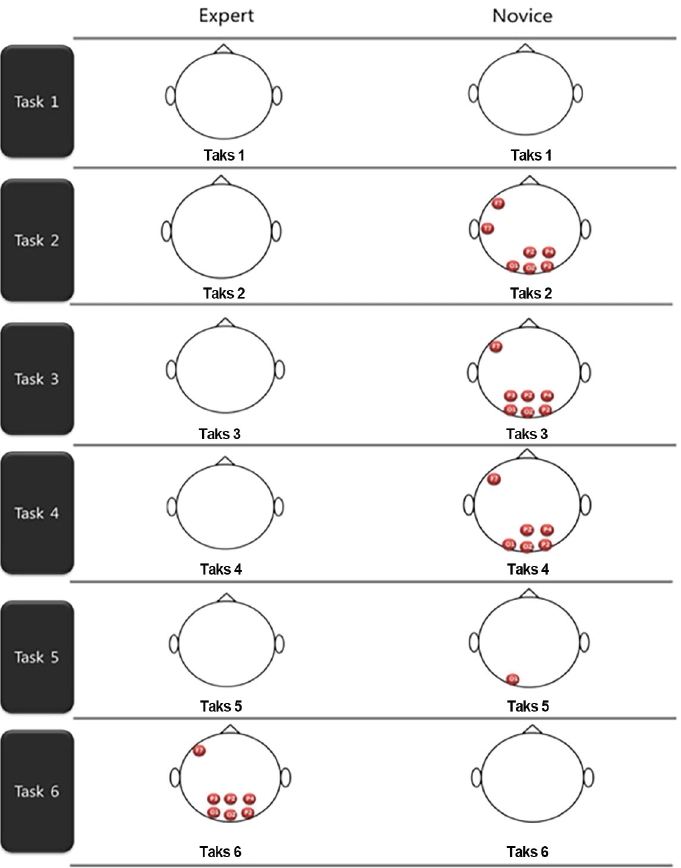
In order to analyze the characteristics during clinical decision-making in the brain, cortical activities were analyzed in 10 experts and 10 novices. As a result, the two groups did not differ in the background signals measured in a relaxed state with the eyes closed, and during the first task (confirmation of the patient’s chief complaints), the novices had higher activities in the left frontal lobe, occipital lobe, and parietal lobe than the experts at the steps where oral examination & radiography reading. After EEG measurement, the accuracy of the participants’ diagnoses made to investigate their clinical decision making was analyzed in order to measure the difficulty of each task. In task 6 (oral examination data), which was difficult and had the lowest accuracy of diagnoses made by the experts, the brain activities in both groups were higher than in other tasks. in particular, the experts’ activities in left frontal lobe, occipital lobe, and parietal lobe were higher than those observed in the novices.
Two sets of tasks were performed for measurement of EEG signals. Set 1 was presented in the order of auditory data, oral photograph, and radiograph of the same patient whereas set 2 was presented in the order of auditory data, oral photograph, and radiograph of three different patients for whom different decisions were required. When differences in tasks within sets and differences between groups and sets were investigated, no statistical significance was noted. However, this study was identified changes in the EEG signals activated for identical stimuli and those activated for different stimuli in each set in a chronological order, as shown in Fig. 4.
The results may be interpreted differently depending on the difficulty of the tasks. For each task, the participants were given time after EEG signal measurement to document with hands the decision-making process used to solve the patient’s problem. In this study, the difficulty of tasks was assessed by statistically analyzing the accuracy of diagnoses made by the experts and novices after measuring EEG signals during clinical decision making. Table 1 demonstrates the groups’ differences. Since this task was more difficult than others, the brain areas would have been activated in the experts to proceed with decision making.
Discussion
This study aims to analyze the differences in clinical decision-making and problem-solving between medical experts and novices and to develop tasks based on processes with significant differences. This study also aimed to measure EEG signals from the participants and analyze the characteristics of brain activation in experts to explore brain-based knowledge models used by experts in clinical decision-making. This study obtained the following conclusions.
As with Wainwright et al. [17], who suggested that expert clinical decision-making is based on comprehensive, organized knowledge, this study also confirmed that clinical problem-solving in experts proceeds based on evidence under a wide range of thinking. However, in contrast to the report that most medical experts make clinical decisions based on forward reasoning, this study observed backward reasoning. The medical experts still differed from the novices in using broad, organized knowledge to make decisions. The experts and novices showed differences in their decision-making in the clinical treatment experiment in history taking, physical examination, and radiography reading stages, so these were selected as the basic frames for tasks in enterprise resource planning to analyze the differences in brain activation between the experts and novices. When differences in cortical activation during clinical decision making were compared between the expert and novice dentists, this study was observed different types of differences. We also confirmed the results of Shallice [18] who suggested that experts have activation in the middle frontal lobe, those of Nichelli et al. [19] who suggested that the prefrontal and parietal lobes are important in experts when compared to novices [20]. Moreover, our results supported other previous studies that performed EEG analysis in chess experts and found that the activation of right frontal, occipital, and parietal lobes is more prominent compared to the left hemisphere [21-24]. This study also found that the activation of EEG signals in the experts was relatively higher when compared to the novices in task 6, which had the highest difficulty, clarifying that the experts also had different cortical activation based on the difficulty of tasks. As suggested by Duncun et al. [25] and Chen et al. [26], both hemispheres were activated when performing higher-order cognitive functions, although the activities differed depending on the tasks being performed [27,28].
MacLean [29] suggested the tribune brain theory and developed a model of brain-based teaching of subjects, and studies have investigated its effects. This study could also associate the function of cortical areas activated during medical experts’ decision-making with teaching and learning. Here, this study is suggested learning directions for brain-based clinical decision-making that can be approached to raise experts based on brain use. First, clinical decision-making training should be provided in which the clinicians can perform backward reasoning and maintain an open mind to other possibilities while recognizing certain information about the patient. Second, Soursa [30] reported that students with different sensory preferences react differently to identical stimuli. Training should discourage using certain brain areas and instead present various learning stimuli and learning formats to enable the use of both brains. Third, by developing education models that offer various patient cases and focus on clinical expressions, stimuli from patient experiences should be maximized, and clinicians should be encouraged to accumulate and integrate experiential knowledge. Fourth, to further activate the parietal lobe, which is responsible for somatosensation and higher-order sensory processing, opportunities to experience more multidimensional tasks than the currently performed tasks should be provided. Fifth, instructional methods that can equally activate the left brain focusing on logical thinking and the right brain focusing on intuitive thinking should be developed and applied to activate both brains.
This study analyzed differences between medical experts and novices in problem-solving and EEG signals during clinical decision-making. It explored a model of clinical decision-making based on brain-based knowledge used by experts in clinical decision-making. Based on the findings, this study developed and suggested a model of the decision-making process for experts and novices and suggested the basic directions for brain-based learning needed to raise experts based on brain activity. This model is expected to serve as findings of basic brain-based research that investigated steps and factors to improve core competency required for clinical decision-making and suggested ways to strengthen accurate clinical decision-making capabilities with little time and effort. Because of limits in methodology, this study could not be conducted on many participants. More extensive samples should be used to generalize the differences in clinical decision-making between experts and novices found in this study, and studies should continue with participants of various backgrounds.